
Best Skincare Ingredients for Sensitive Skin: A Dermatologist-Backed Clinical Guide
The ingredients with the strongest clinical evidence for sensitive skin are ceramides paired with cholesterol and fatty acids (in the physiologic 3:1:1 ratio), niacinamide at 2–5%, colloidal oatmeal (an FDA Category I skin protectant), panthenol, glycerin, and zinc oxide or titanium dioxide mineral sunscreen. Together, they address every major driver of skin sensitivity: lipid barrier loss, inflammatory signaling, dehydration, and sensory nerve hyperreactivity. Everything else in most sensitive-skin routines is supporting cast.
This guide draws on peer-reviewed dermatology literature, FDA monograph data, and barrier-repair research — not brand partnerships or marketing claims. If you have rosacea, eczema, perioral dermatitis, or symptoms that don’t improve with consistent barrier care, a board-certified dermatologist can rule out conditions that mimic sensitive skin but respond to entirely different treatments.
What “Sensitive Skin” Actually Means — And Why Most Advice Gets It Wrong
About half of adults describe their skin as sensitive when asked directly. That number tells you two things: this is one of the most common skin concerns in the world, and it’s almost certainly being oversimplified in most of the content written about it.
“Sensitive skin” isn’t a single diagnosis. It’s the surface-level output of several distinct biological mechanisms, and they don’t all respond to the same fix. A routine built around “gentle” as a feeling will always underperform a routine built around which mechanism is actually driving your symptoms.
The four main mechanisms:
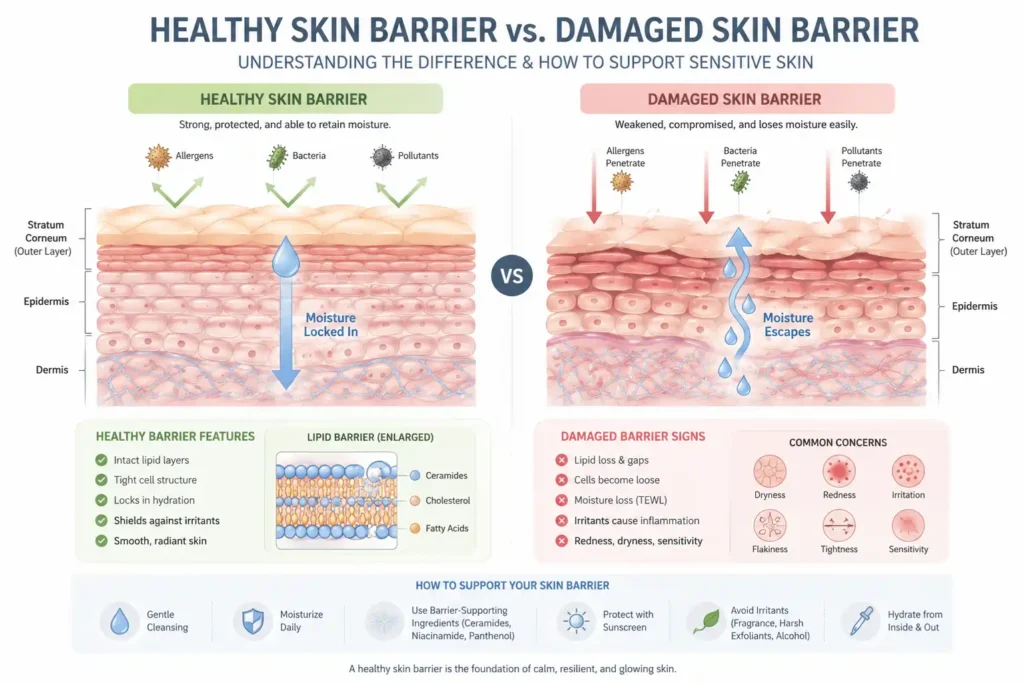
1. Lipid barrier dysfunction. The outermost skin layer (stratum corneum) is held together by lipids — primarily ceramides, cholesterol, and fatty acids — arranged in a tightly packed lamellar structure. When that structure is depleted or disrupted, water escapes and irritants enter more easily. The result is tightness, flaking, and heightened reactivity to products that were previously tolerated without issue.
2. Sensory nerve hyperreactivity (the TRPV1 pathway). This is the mechanism most sensitive-skin content skips entirely, and it explains the most confusing version of the problem: skin that stings or burns from products with seemingly harmless ingredient lists. A receptor called TRPV1 sits on sensory nerve endings, keratinocytes, and mast cells throughout the skin. When sensitized, it triggers the release of neuropeptides — substance P and CGRP — that cause burning, itching, and visible redness even without measurable barrier damage beneath the skin. This is neurogenic inflammation, and it requires different ingredients to calm than barrier repair alone provides.
3. Chronic low-grade inflammation. Some skin reactivity isn’t an acute response to a specific product — it’s a background state of inflammatory signaling that makes the skin hair-trigger reactive to almost everything. This can be driven by the microbiome, UV damage, hormonal shifts, or immune factors. It’s worth understanding that stress is also a documented trigger that worsens pre-existing skin conditions, including chronic sensitivity.
4. Dehydration-driven sensitivity. Skin that lacks water becomes rigid and irritable. This is separate from lipid barrier loss (which causes water to escape) and requires humectant-based hydration, not just more oil or emollient.
Why this matters: stacking five “calming” serums that all address the same mechanism while leaving one of the other three untouched is the most common formulation mistake in sensitive-skin routines. You may genuinely be using good products and still getting poor results.
Sensitive Skin vs. Rosacea vs. Eczema vs. Contact Dermatitis vs. Perioral Dermatitis: A Clinical Distinction That Changes Everything
Before choosing ingredients, it helps to rule out conditions that sensitive skin is routinely mistaken for — because some habits that help with general sensitivity can actively worsen others.
| Condition | Hallmark Pattern | The Mistake Most People Make |
|---|---|---|
| Sensitive skin | Stinging, burning, or tightness after product contact; no persistent rash | Treating it like acne and adding more actives |
| Rosacea | Persistent central facial redness, visible vessels, flushing from heat, alcohol, or spice | Using physical scrubs or strong exfoliating acids, both of which worsen flushing |
| Eczema (atopic dermatitis) | Dry, itchy, poorly defined patches; often starts in childhood; flares seasonally | Hot showers and fragranced “soothing” lotions, which strip lipids |
| Contact dermatitis (irritant or allergic) | Reaction confined to where a specific product touched the skin | Continuing the product because “it usually works fine” |
| Perioral dermatitis | Small red bumps clustered around the mouth, sparing a clear margin at the lip line; can extend to the nose or eyelids | Reaching for heavier moisturizer or a topical steroid — both are documented triggers |
Perioral dermatitis deserves more attention than it gets in most sensitive-skin content. It affects mostly women between 16 and 45, is frequently misdiagnosed as eczema or acne, and is specifically worsened by the instinctive responses to “sensitive” skin — heavy occlusive creams, topical steroids, and fluoridated toothpaste are all established triggers. If your sensitivity presents as clustered bumps that respect the lip border, more moisturizer is the wrong move. Simplifying to a single fragrance-free, non-occlusive cleanser and moisturizer — and seeing a dermatologist if it persists — is the correct one.
The Biological Infrastructure Behind Sensitive Skin: Three Systems Most Guides Ignore
The Acid Mantle: Your Skin’s pH Is Not a Wellness Trend
The healthy skin surface sits at a mildly acidic pH of roughly 4.5–5.5. This isn’t cosmetic trivia — it governs everything from how your ceramides are processed into their finished, barrier-ready form to how quickly dead skin cells release from the surface (desquamation). Push the pH up, which alkaline soap does for as long as 90 minutes per wash, and those enzyme systems slow down or stop working efficiently.
This is one of the most overlooked reasons so-called “gentle” foaming cleansers still leave reactive skin feeling tight: foaming surfactants are frequently alkaline, and the irritation shows up hours after rinsing, not during it. If your cleanser produces a rich foam and leaves your skin feeling squeaky, it’s a reasonable first suspect — switch to a cream or low-foam cleanser formulated at a pH near 5 before troubleshooting anything else. Our guide to the best organic cleansers for sensitive skin covers several pH-appropriate options worth considering.
The Skin Microbiome: A Barrier Participant, Not a Passenger
Staphylococcus epidermidis, one of the dominant bacteria on healthy skin, manufactures ceramides and antimicrobial peptides that directly reinforce the lipid barrier. When the barrier is compromised, the microbial balance shifts: atopic dermatitis skin shows Staphylococcus aureus overcolonization in roughly 90% of cases alongside a measurable drop in microbial diversity. Rosacea-prone skin exhibits a distinct pattern involving Demodex mites and Bacillus oleronius.
Understanding what the skin microbiome is and how to protect it is the missing piece in most conversations about sensitivity. Over-cleansing or alcohol-based toners can deepen sensitivity over time, even when they feel “clean” in the moment — they don’t just strip lipids; they disrupt the bacterial ecosystem that helps maintain them. Ceramide-rich moisturizers and colloidal oatmeal both support a stable surface environment and consistently outperform aggressive antibacterial cleansing for reactive skin in clinical outcomes.
The TRPV1 Nerve Pathway: Why Skin Stings When Nothing Is Visibly Wrong
When TRPV1 is activated, neuropeptides flood the skin, producing burning and redness without an allergic mechanism or underlying structural damage. The triggers can be subtle: a slight pH drop, a temperature change, menthol, certain preservatives, or low-molecular-weight alcohols — acting on an already sensitized nerve pathway rather than on the barrier itself.
This matters because it means barrier repair alone is often not enough. TRPV1-driven sensitivity needs ingredients with documented calming effects on nerve-level reactivity, specifically: panthenol, colloidal oatmeal’s avenanthramides, and centella asiatica’s triterpenes, all of which have evidence here, not just for patching the lipid matrix.
Quick Self-Assessment: Which Mechanism Is Driving Your Sensitivity?
This is not a diagnostic tool — only a dermatologist can diagnose a skin condition — but it helps you decide where to start.
| If your skin mostly… | The likely primary driver | Start here |
|---|---|---|
| Feels tight, flaky, rough, and reacts worse in winter | Barrier/lipid depletion | Ceramide-cholesterol-fatty acid moisturizer twice daily |
| Stings within seconds of applying almost anything, including plain water | TRPV1 nerve hyperreactivity | Panthenol + colloidal oatmeal, eliminate all fragrance |
| Reacts only to specific products, in the exact area of application | Contact dermatitis (irritant or allergic) | Stop the product; patch test before reintroducing anything |
| Shows clustered bumps around the mouth that spare the lip margin | Possible perioral dermatitis | Simplify drastically; see a dermatologist if it persists in 4 weeks |
| Flushes with heat, alcohol, or spicy food; visible vessels present | Possible rosacea | Dermatologist evaluation; azelaic acid is a reasonable first step |
The Best Skincare Ingredients for Sensitive Skin, Ranked by What They Actually Fix
If you want a broader view of which top skincare ingredients actually work across all skin types, our guide is worth reading alongside this one. Here, we focus on the specific subset with the strongest evidence for reactive, sensitive skin.
Ceramides: The Structural Material Your Barrier Is Built From
Ceramides are not a single ingredient. There are at least nine identified lipid subtypes in human skin, and the differences between subtypes matter more than most skincare marketing acknowledges.
| Subtype | Primary Role | Why It Matters for Sensitive Skin |
|---|---|---|
| Ceramide NP | Most abundant subtype in healthy stratum corneum (roughly 20% of total ceramide content) | The foundational barrier lipid, nearly every effective formula includes it |
| Ceramide AP | Anti-inflammatory activity | Specifically useful for reactive, redness-prone skin, not just dry skin |
| Ceramide EOP | Anchors the lamellar (layered) lipid structure | Measurably depleted in eczema-affected skin, making it a priority for chronically reactive skin |
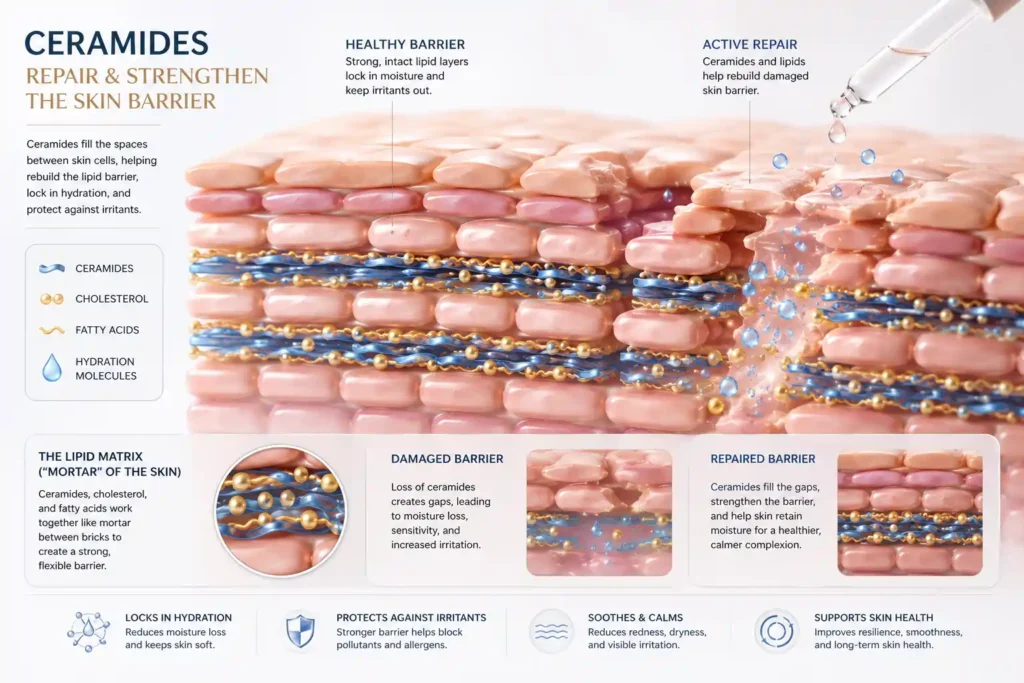
Ceramides function best alongside cholesterol and free fatty acids in roughly a 3:1:1 ratio — called the “physiologic” or skin-identical ratio because it mirrors the proportions found in healthy stratum corneum. A ceramide-only product without the other two lipid types is structurally incomplete. Think of it as rebuilding a brick wall with bricks but no mortar.
When reading a label, don’t stop at the word “ceramide” on the front. Look for cholesterol and fatty acids (stearic acid, linoleic acid, palmitic acid) listed alongside the ceramide in the INCI ingredient list. That combination — not the marketing claim — is the real quality signal.
If you’re trying to decide between ceramide vs niacinamide for skin barrier repair, the short answer is that you don’t have to — they work better together than apart. Read our detailed guide on it.
A 2023 review in Skin Pharmacology and Physiology, co-authored by Northwestern University dermatologist Dr. Peter Lio, concluded that moisturizers built on this multi-lipid model outperform single-ingredient barrier repair across atopic and irritant-driven skin conditions. That’s a meaningfully stronger evidence base than most ingredient claims in this category can cite.
How long until you see results? Most people notice measurable improvement in texture and reduced reactivity within 2–4 weeks of consistent twice-daily use of a ceramide-cholesterol-fatty acid moisturizer, with continued gains through 6–8 weeks. Barrier lipid turnover is a slow biological process — rotating products before giving any one formulation that window is one of the most common reasons people never find a moisturizer that “works.”
Niacinamide for Sensitive Skin: What It Actually Does at the Cellular Level

Niacinamide (vitamin B3) earns its position because it does two jobs usually treated as separate problems. It measurably increases the skin’s own ceramide synthesis — meaning it supports your skin in manufacturing more of its own barrier lipids, rather than only supplying them topically — and it independently dampens the inflammatory signaling that drives chronic redness.
The concentration question has a clear, evidence-based answer: 2–5% is the range used in clinical research demonstrating these benefits. Above 5%, you’re paying for a number on the label, not better outcomes. At 10% or higher, the risk of a transient flushing or stinging reaction increases meaningfully in already-sensitized skin, particularly in poorly buffered formulas or those that also contain zinc PCA.
For a curated list of formulas that get this right, see our picks for the best niacinamide serums for sensitive skin.
If a niacinamide serum irritates you, the fix usually isn’t to avoid niacinamide altogether — it’s to drop it to 4% or lower and scrutinize the rest of the formula. Fragrance and high denatured alcohol content are far more often the actual culprits than the niacinamide itself.
And if rosacea is part of your picture, our guide on whether niacinamide is bad for rosacea addresses that nuance directly.
Do niacinamide and vitamin C cancel each other out?
The long-standing claim that they must be used at separate times has not held up under modern formulation review. The real limiting factor for sensitive skin is whether the vitamin C formula itself (typically low-pH and more acidic) is tolerated on its own — not an inherent interaction between the two actives.
Our deep dive on vitamin C vs niacinamide walks through exactly when to use each and when to use both.
Colloidal Oatmeal: The Only Ingredient Here With a Federal Drug Classification
Colloidal oatmeal is not a wellness trend. It is a regulated OTC drug ingredient. Under FDA Skin Protectant Monograph M016, colloidal oatmeal is recognized as a Category I skin protectant for the temporary relief of minor skin irritation and itching from eczema, rashes, and insect bites. That classification exists because of its mechanism, not its reputation.

The mechanism is multi-layered. Oatmeal’s polysaccharides form a hydrocolloid film that physically slows water loss. Its beta-glucan content supports moisture retention. A class of compounds unique to oats called avenanthramides has documented anti-inflammatory and antioxidant activity that directly calms the nerve-level itching described above — making oatmeal one of the few topical ingredients with evidence for addressing TRPV1-driven sensitivity, not just structural barrier repair.
For facial use, leave-on oatmeal creams provide more sustained benefit than oatmeal baths, which rinse away rather than maintaining the protective film. The exception worth stating clearly is that true oat allergy exists and is distinct from gluten sensitivity. If you have a documented oat allergy, this is one of the rare ingredients to avoid outright rather than simply patch-test.
Hyaluronic Acid, Polyglutamic Acid, Glycerin, and Urea: Humectants Are Not Interchangeable
All four attract or retain water, but they work differently and suit different situations.
| Humectant | How It Works | Best For | Key Limitation |
|---|---|---|---|
| Glycerin | Strong water attraction; decades of tolerability data | Nearly all sensitive skin types; most universally tolerated humectant | Feels tacky at high concentrations in humid climates |
| Hyaluronic acid | Binds water within upper skin layers; different molecular weights penetrate differently | Dehydration-driven tightness | In very low-humidity environments, can pull moisture from deeper skin layers if not sealed with an occlusive |
| Polyglutamic acid | Forms a surface film that slows water evaporation | An added moisture-retention step layered under HA | Newer ingredient; less long-term clinical data than glycerin or HA |
| Urea (2–10%) | Natural Moisturizing Factor component; mild keratolytic at low concentration | Rough, flaky texture alongside dryness | Concentrations above 10% are exfoliating, not just hydrating — too aggressive for reactive facial skin |
The critical mistake sensitive-skin routines most often make
A humectant without a sealing moisturizer on top can leave skin drier, especially in low-humidity environments, because humectants pull water from wherever it’s available — including, in dry air, from deeper skin layers — and then have nothing to prevent evaporation from the surface.
Hyaluronic acid serum used alone, with no ceramide moisturizer layered over it, is one of the most common self-inflicted causes of “this product made my skin worse” complaints. The serum is not the problem. The missing occlusive is.
Panthenol (Pro-Vitamin B5): The Most Underrated Ingredient for Reactive Skin
Panthenol converts to pantothenic acid in the skin and supports barrier function, hydration, and visible recovery after skin stress. It’s the default ingredient in post-procedure products used after chemical peels, laser treatments, and microneedling — precisely because it accelerates barrier recovery without increasing the risk of irritation.
For sensitive skin specifically, panthenol is valuable less for what it adds and more for what it doesn’t do: it has essentially no track record of triggering stinging, sensitization, or the kind of low-level inflammatory response that niacinamide at high concentrations, vitamin C, or fragrance occasionally cause. Pairing panthenol with ceramides is one of the few ingredient combinations in skincare where the clinical rationale (one repairs structure, the other supports the cellular environment for repair) and the real-world tolerability story actually line up consistently.
Centella Asiatica, Green Tea, and Botanical Soothers: Where the Evidence Is Real — and Where It Isn’t
Not every “calming” plant extract belongs in the same sentence. Here’s how the evidence actually stacks up:
Centella asiatica (Cica): Contains three well-studied compounds — madecassoside, asiaticoside, and asiatic acid — with documented effects on wound healing and inflammatory signaling. Among botanical soothers, centella has the most mechanistically grounded support for barrier-compromised, reactive skin.
Green tea extract (EGCG): Real antioxidant and anti-inflammatory data exist, though the evidence is stronger for environmental protection than for treating active irritation. A valuable addition for UV-stressed sensitive skin; not a substitute for barrier repair.
Aloe vera: Genuinely soothing for short-term, mild irritation (sunburn, minor friction). Does not have sufficient evidence for barrier repair or nerve calming to make it a primary active for chronic sensitivity.
The category-wide warning most content states but doesn’t follow through on
“Natural” and “gentle” are not synonyms. Essential oils, fragrance components, and numerous botanical extracts are among the most common cosmetic allergens documented by the American Academy of Dermatology — precisely because plant-derived compounds are chemically complex and highly variable.
Before reaching for a botanically rich formula, it’s worth understanding how essential oils interact with different skin types, since what soothes one skin type can actively inflame another. A lavender-infused “calming serum” is, mechanistically, closer to a fragrance product than to a centella product.
Mineral Sunscreen Ingredients for Sensitive Skin: Zinc Oxide vs. Titanium Dioxide
| Zinc Oxide | Titanium Dioxide | |
|---|---|---|
| UVA protection | Broader spectrum; generally the stronger UVA filter | Good UVB coverage; narrower UVA range |
| Sensitive skin tolerance | Excellent; the default for reactive and eczema-prone skin | Excellent; often combined with zinc oxide for full-spectrum coverage |
| Texture | Can appear thicker or whiter unless micronized | Slightly easier to formulate into lighter textures |
| FDA status | Recognized as generally safe and effective for OTC sunscreen use | Recognized as generally safe and effective for OTC sunscreen use |

Daily SPF 30+ is not optional for sensitive skin. Unrepaired UV damage is itself a barrier disruptor and a documented driver of the chronic low-grade inflammation that makes skin more reactive over time. For sensitive skin specifically, mineral filters remain the safer default, not because chemical filters are inherently unsafe, but because their physical-filtering mechanism produces far fewer reports of stinging — particularly around the eyes, where chemical filters are most problematic.
Our guide to the best sunscreen ingredients for sensitive skin goes deeper into this comparison, and if rosacea is a factor, the top zinc oxide sunscreens for rosacea are worth a look.
For anyone still unsure whether to go with a physical or chemical approach, a clear breakdown of the pros and cons of each can help you make a more informed decision.
Ingredients to Avoid if You Have Sensitive Skin (And How to Find Them on a Label)
The INCI list — the standardized International Nomenclature of Cosmetic Ingredients that regulators require on every product — is the only part of a skincare label legally required to be accurate. “Clean,” “gentle,” “natural,” and ” dermatologist-tested ” are unregulated marketing terms. The INCI list is where the real information lives.
| What to Avoid | How It Appears on the INCI List | Why It Causes Problems |
|---|---|---|
| Fragrance | “Fragrance,” “Parfum,” “Perfume,” named essential oils (lavender oil, rose oil, etc.) | The single most common cosmetic allergen category identified by the AAD |
| Drying alcohols | “Alcohol Denat.,” “SD Alcohol,” “Isopropyl Alcohol” — not cetyl or stearyl alcohol, which are beneficial fatty alcohols | Volatile alcohols increase transepidermal water loss and disrupt surface lipids |
| Sodium lauryl sulfate (SLS) | “Sodium Lauryl Sulfate” — note that sodium laureth sulfate is meaningfully milder | Used as a standard irritant in barrier research precisely because of how reliably it disrupts the lipid matrix |
| Stacked exfoliants | Multiple named acids (glycolic, lactic, salicylic, mandelic) are used simultaneously | Cumulative over-exfoliation is the most common self-induced cause of acquired sensitivity |
| High-strength actives introduced abruptly | Any retinoid or acid formula without low-strength entry options | Gradual introduction consistently outperforms aggressive starts in barrier-compromised skin |
The distinction between fatty alcohols and drying alcohols is frequently misunderstood. Cetyl alcohol, stearyl alcohol, and cetearyl alcohol are emollient, skin-conditioning fatty alcohols — they’re beneficial, not harmful. The ones to avoid are the small, volatile molecules: alcohol denat., SD alcohol and isopropyl alcohol evaporate, pulling water with them.
Anti-Aging Skincare Ingredients That Won’t Destroy a Sensitive Barrier
The instinct to avoid all actives when skin is reactive costs real results. The better approach is to match the active to your actual tolerance ceiling and introduce it properly.
Bakuchiol is the most reasonable entry point for retinoid-intolerant skin. A randomized controlled trial published in the British Journal of Dermatology found that bakuchiol produced improvements in fine lines and pigmentation comparable to those of retinol, with significantly fewer reports of scaling and stinging. It is not a retinol substitute in mechanism, but it is a legitimate substitute in terms of outcomes for people who cannot tolerate retinoids at all.
Azelaic acid occupies a unique position in sensitive-skin care: it is anti-inflammatory, mildly antibacterial, and evens skin tone — and unlike most exfoliating acids, it is specifically well tolerated by rosacea-prone and redness-prone skin because the American Academy of Dermatology recognizes it as a clinically proven rosacea treatment, not merely an acne ingredient. Starting at 10% over-the-counter formulas and pairing with a ceramide moisturizer measurably improves tolerability during the first few weeks.
If hyperpigmentation is part of your concern alongside sensitivity, our guide to azelaic acid for hyperpigmentation and the real-world azelaic acid before-and-after results are useful companion reads.
Peptides are signaling molecules, not exfoliants. They carry a much lower irritation profile than retinoids or acids while still supporting collagen-related outcomes over time — a reasonable anti-aging addition for mature sensitive skin that needs the benefit without an adjustment period. Our ultimate guide to peptide serums covers the seven key anti-aging benefits and how to layer them without disrupting a sensitive routine.
Retinoids are not categorically off-limits for sensitive skin — but entry strategy matters more here than for any other skin type. The realistic tolerability gradient runs: retinyl esters (gentlest, weakest) → retinol (moderate, most studied) → retinaldehyde → tretinoin and prescription retinoids (strongest, most irritating). Understanding how retinol works at the cellular level helps set realistic expectations about the adjustment period and why starting low and slow actually produces better long-term results. Starting at the wrong end of that ladder is the single most common reason people conclude “I just can’t use retinol,” when a lower rung, used two nights per week under a ceramide moisturizer, might have worked fine.
On skin cycling: the trend of rotating exfoliant nights, retinoid nights, and recovery nights has genuine logic — it provides deliberate time for barrier recovery. But for truly reactive skin, even the “recovery” nights in most skin-cycling templates assume a baseline tolerance that sensitive skin often doesn’t have. Extend the recovery phase to two or three nights rather than one, and don’t introduce a new active until the previous one has been tolerated without reaction for at least two full weeks.
Our guide on how to layer skincare actives without irritation provides a practical sequencing framework for exactly this situation.
Skincare Routine for Sensitive Skin: Morning and Night, by Subtype

Morning Routine for Sensitive Skin
- Gentle, low-pH cleanser — non-foaming, cream or micellar, no sulfates or fragrance
- Hydrating serum — glycerin, panthenol, or low-molecular-weight hyaluronic acid
- Barrier-repair moisturizer — ceramide + cholesterol + fatty acid formula; apply while skin is slightly damp
- Mineral SPF 30+ — zinc oxide or titanium dioxide, fragrance-free
Evening Routine for Sensitive Skin
- Same gentle cleanser
- Optional active (only after barrier is stable) — niacinamide 4%, azelaic acid 10%, or low-strength retinoid 2–3×/week
- Same barrier-repair moisturizer — applied generously; this is when skin does most of its repair work
Routine by Sensitive Skin Subtype
| Subtype | Morning Priority | Evening Priority | Avoid |
|---|---|---|---|
| Dry sensitive | Rich ceramide cream + mineral SPF | Same cream, applied generously | Foaming cleansers, high-strength urea |
| Oily sensitive | Niacinamide serum + lightweight ceramide lotion + mineral SPF | Niacinamide, gel or lotion texture | Heavy occlusive balms |
| Acne-prone sensitive | Niacinamide + non-comedogenic ceramide moisturizer + mineral SPF | Azelaic acid 2–3×/week + ceramide moisturizer | Combining azelaic acid with other exfoliating acids on the same night |
| Rosacea-prone | Azelaic acid + ceramide moisturizer + mineral SPF | Ceramide moisturizer, niacinamide | Physical scrubs, alcohol toners, and very hot water |
| Aging sensitive | Peptide serum + ceramide moisturizer + mineral SPF | Low-strength retinoid (2–3×/week) under ceramide moisturizer | Jumping to prescription-strength retinoids without tolerating lower rungs first |
| Perioral dermatitis-prone | Non-foaming cleanser only; minimal layering | Same cleanser + lightweight non-occlusive moisturizer only | Heavy creams, topical steroids, and fluoridated toothpaste near the area |
Ingredient Pairings That Work Synergistically
Ceramides + Cholesterol + Fatty Acids: Mirrors the skin’s own lamellar lipid structure. The most clinically supported combination in barrier-repair science. Do not use ceramides alone without the other two components.
Niacinamide + Hyaluronic Acid: Niacinamide supports barrier function from the inside (lipid synthesis, anti-inflammatory signaling); HA addresses hydration at the surface level. Different mechanisms, complementary results.
Panthenol + Colloidal Oatmeal: Panthenol accelerates barrier recovery; oatmeal’s avenanthramides calm nerve-level reactivity. One of the most useful combinations specifically for TRPV1-driven stinging sensitivity.
Azelaic Acid + Ceramide Moisturizer: The moisturizer helps buffer the mild dryness that azelaic acid can cause during the first two to three weeks of use and significantly improves tolerability for rosacea-prone and sensitive skin. For those also dealing with acne, our comparison of niacinamide vs azelaic acid for acne clarifies when to use each and when to combine them.
Polyglutamic Acid + Glycerin: PGA slows water evaporation from the surface while glycerin attracts water into the skin. Layering them gives both mechanisms simultaneously without the risk of either one working against the other.
The 30-Day Barrier Reset Protocol
A genuinely damaged barrier — flaking, persistent tightness, reactive to nearly everything — usually doesn’t need a new product. It needs fewer products and more time. For a fully detailed, step-by-step approach, our guide on repairing a damaged skin barrier expands on everything below.
Days 1–7 — Strip down. Cut your routine to a non-foaming cleanser and a ceramide-cholesterol-fatty acid moisturizer, morning and night, plus mineral SPF during the day. No actives. No serums. No exfoliants. This phase exists to prevent the introduction of new variables while the barrier has uninterrupted time to rebuild.
Days 8–14 — Add hydration support. If skin is stable (no new stinging, redness trending down), layer in a glycerin- or panthenol-based hydrating step under the moisturizer. This is also the earliest reasonable point to reintroduce niacinamide at 4% or lower if redness or texture issues remain.
Days 15–21 — Reassess, don’t rush. Most barrier repairs become apparent in this window. If the skin is calm, this is the earliest point to patch-test one additional active — not to add it to the full face.
Days 22–30 — Reintroduce one active at a time, on its own week. Whether that’s a low-strength retinoid, azelaic acid, or a gentle exfoliant — introduce exactly one, at the lowest available strength, two to three nights per week. Hold everything else steady. Adding two new things in the same week is the most common reason people can’t identify their own triggers months later.
How to Patch Test New Skincare Products Properly
Most people patch-test for 30 minutes, declare success, and apply the product to their entire face — only to wonder why they’re reacting three days later. Here’s how to do it in a way that actually catches both types of reactions.
- Apply a small amount to the inner forearm or behind the ear — not the jawline, where irritation is more visible and harder to conceal.
- Leave it in place as the product’s instructions direct, without immediately rinsing the area.
- Watch for 7–10 days, not just the first hour. Allergic-contact reactions typically take 48–96 hours to appear. Irritant reactions show up more immediately. Testing for only a few minutes catches neither reliably.
- Stop immediately if you see persistent redness, swelling, blistering, or intense itching. Do not “push through” — sometimes skin adjusts, but there’s no reliable way to predict which reactions will resolve and which will worsen.
Special Situations Most Sensitive-Skin Guides Don’t Cover
Pregnancy: Several commonly recommended actives are typically avoided during pregnancy — most notably retinoids (including topical retinol) and high-dose salicylic acid. Ceramides, niacinamide, azelaic acid, colloidal oatmeal, glycerin, and mineral sunscreen are generally considered pregnancy-compatible barrier-support choices.
For those specifically dealing with pigmentation changes during pregnancy, our guide on azelaic acid for melasma covers the safety profile in detail.
Always confirm specific activities with your OB-GYN or dermatologist.
Skin of color: Sensitive skin in deeper skin tones carries a meaningfully higher risk of post-inflammatory hyperpigmentation after any irritation. The visible consequence of a reaction often outlasts the reaction itself by months. Patch testing and gradual active introduction matter even more in this context, not less.
Men and daily shaving: Shaving is a mechanical barrier disruptor that interacts with sensitivity differently than it does for non-shaving skin. Razor burn and post-shave sensitization are frequently mistaken for inherent skin sensitivity when the actual driver is technique and a missing post-shave barrier step — a ceramide-based balm, not an alcohol-based aftershave.
Children: Children’s skin barrier is still maturing and has a higher surface-area-to-body-weight ratio, meaning proportionally greater topical absorption. Default to fragrance-free, minimal-ingredient formulations and avoid adult-strength actives rather than diluting them.
Post-cancer treatment: Chemotherapy and radiation frequently induce pronounced barrier dysfunction with heightened sensitivity to fragrance, friction, and sun exposure. The barrier-reset protocol above — minimalist, fragrance-free, ceramide- and panthenol-forward — generally applies here, often providing a longer stabilization window than typical for sensitive skin.
Seasonal Adjustments for Sensitive Skin
Winter: Cold air holds less moisture. Transepidermal water loss increases even before wind or indoor heating is factored in. Barrier-dependent sensitivity reliably worsens. Lean toward richer ceramide moisturizer textures and pull back on exfoliating actives during the coldest months.
Our ultimate guide to building a winter skincare routine covers the full seasonal shift for reactive skin, and the winter skincare essentials expert guide offers specific product-category recommendations.
Summer: Higher ambient humidity reduces water loss but adds UV load and sweat-related irritation. Shift priority toward consistent mineral SPF reapplication and lighter-textured ceramide formulas — not abandoning ceramides, but choosing gel or lotion versions over heavy creams that can feel suffocating in heat.
Frequently Asked Questions: Best Skincare Ingredients for Sensitive Skin
What skincare ingredients are best for sensitive skin?
Ceramides paired with cholesterol and fatty acids, niacinamide at 2–5%, colloidal oatmeal, panthenol, glycerin, and zinc oxide or titanium dioxide sunscreen. These address the four core mechanisms: lipid barrier loss, inflammatory signaling, dehydration, and nerve-level reactivity.
What is the safest niacinamide percentage for sensitive skin?
2–5%. This is the concentration range used in clinical research demonstrating barrier and anti-inflammatory benefits. Concentrations above 10% increase the risk of irritation without meaningful additional benefit.
Is hyaluronic acid bad for sensitive skin in dry climates?
Not inherently, but it’s incomplete when used alone. Without an occlusive moisturizer layered on top, a humectant in low-humidity air can pull moisture from deeper skin and allow it to evaporate — leaving skin drier than before application. The answer is to seal it, not skip it.
How long does it take for ceramides to repair the skin barrier?
Most people see measurable improvement in 2–4 weeks of consistent twice-daily use, with continued gains through 6–8 weeks. Barrier lipid turnover is a slow biological process — the most common mistake is rotating products before giving any single formulation a chance to work.
Can I use retinol with sensitive skin?
Often yes — but starting strategy matters more than for any other skin type. Begin with the lowest available strength, two to three nights per week, always applied under a ceramide moisturizer. The most common reason people conclude retinoids “don’t work for their skin” is starting too high, too often, too fast.
What is the #1 dermatologist-recommended brand for sensitive skin?
There is no universal consensus recommendation. CeraVe, Vanicream, La Roche-Posay, Avène, and Cetaphil appear most consistently across dermatologist recommendations because their core formulas are built around ceramide-cholesterol-fatty acid barrier repair and are fragrance-free throughout — a formulation philosophy, not brand loyalty.
What should a 70-year-old woman use to wash her face?
A non-foaming, low-pH cleanser that does not strip natural oils. Lipid production declines significantly with age, making older skin more vulnerable to over-cleansing than younger skin. Pair it with a ceramide and panthenol moisturizer; mature skin generally tolerates and benefits from richer textures.
Can colloidal oatmeal cause an allergic reaction?
Yes, though true reactions are uncommon relative to fragrance or essential oil reactions. Anyone with a documented oat allergy should avoid colloidal oatmeal in skincare specifically — not just in food — and consult a healthcare provider before use.
What is the fastest realistic way to repair a damaged skin barrier?
There is no reliable 48-hour fix. The fastest, most consistent path is the 30-day reset described above: strip the routine down to a non-foaming cleanser, a ceramide-cholesterol-fatty acid moisturizer, and a mineral SPF for at least one week before reintroducing anything else. Biological barrier repair operates on a weeks-long timescale, not a days-long one.
The Bottom Line on Sensitive Skin Ingredients
Sensitive skin responds to mechanism-matched ingredients, not to the word “gentle” on a label.
Ceramides rebuild structure. Niacinamide restores function and reduces inflammation. Humectants restore water — but only when sealed in by an occlusive. Panthenol and colloidal oatmeal calm the nerve-level reactivity that barrier repair alone doesn’t reach. Mineral sunscreen protects the progress that everything else makes.
Used in the right combinations, introduced one at a time, and given real weeks rather than days to work, that short list will outperform almost any routine built around chasing the next “calming” serum. And it will tell you — with actual evidence from your own skin, not marketing copy — which mechanism was driving the problem in the first place.

About Subhan Usafzai
Skincare Writer, Researcher & Formulation Specialist
Welcome to my skincare blog! I'm Subhan Usafzai, a passionate skincare enthusiast with over 18 years of experience exploring and learning about all things skin. Join me as I share my tried-and-true tips, product insights, and skincare wisdom.
✅ Medically reviewed by Dr. KhurramKhan, MD, Board-Certified Dermatologist · 📅 Last updated: June 2026
📋 Medical Disclaimer
For Educational Purposes Only: This article is written by Subhan Usafzai, a Medical Writer and Researcher, and is intended for informational and educational purposes only. The content provided is based on scientific research, peer-reviewed studies, and dermatological literature available as of December 2025.
Not Medical Advice: The information in this article does not constitute medical advice, diagnosis, or treatment recommendations. It should not be used as a substitute for professional medical consultation, diagnosis, or treatment from a board-certified dermatologist or qualified healthcare provider.
Individual Results May Vary: Skin conditions, including hyperpigmentation, melasma, and UV-induced pigmentation, vary significantly between individuals based on genetics, skin type, hormonal factors, and environmental exposure.
Consult Your Healthcare Provider: Before starting any new skincare regimen, especially if you are pregnant, breastfeeding, have diagnosed skin conditions, are taking medications, have sensitive skin, or are undergoing dermatological treatments.
Product Safety: Always perform a patch test before using new skincare products. Discontinue use and consult a healthcare professional if you experience irritation or adverse reactions.